
If you’ve been on my website before, or if you’ve read my blog, then you know that one of my major goals is to try and change how doctors think about treating thyroid-related issues.
My personal belief is that patients do not benefit from the archaic treatment paradigm which focuses solely on TSH.
Today I want to dig into that topic a little bit further and talk about how doctors look at TSH, what it actually means, and why we treat the thyroid differently from all other hormone systems in the body.
DOWNLOAD FREE RESOURCES
Foods to Avoid if you Have Thyroid Problems:
I’ve found that these 10 foods cause the most problems for thyroid patients. Learn which foods you should avoid if you have thyroid disease of any type.
The Complete List of Thyroid Lab tests:
The list includes optimal ranges, normal ranges, and the complete list of tests you need to diagnose and manage thyroid disease correctly!
Thyroid Testing and the TSH
As you probably know, doctors tend to look solely at the TSH when they are determining how your thyroid is functioning (1).
This isn’t necessarily a problem by itself, but it should cause some alarm bells to go off once people start realizing that this treatment doesn’t always deliver the results people are looking for.
What do I mean?
When I first started training I found out fairly quickly that thyroid patients tend to be very difficult to treat.
From a conventional standpoint, they don’t ever seem to get better! (Obviously, this isn’t true knowing what I know now, but in the beginning, this is how I felt).
They would come into my office complaining of fatigue or just not feeling like themselves and I would quickly diagnose them with hypothyroidism when their TSH came back as “high”.
The only problem?
The symptoms wouldn’t go away once they were “treated” and their TSH was lowered back to normal.
This didn’t sit well with me from a logical standpoint.
I knew that fatigue was one of the major side effects of hypothyroidism, so wouldn’t it make sense that this fatigue should resolve once the main problem was treated?
It’s always possible that their fatigue could be from some other cause, but I started to second guess my personal bias in regards to treatment when I saw this trend happening over and over.
It caused me to reflect on the TSH as a marker of thyroid function and compare that to how we look at other hormone systems in the body (by we I am referring to doctors).
And I realized that we treat the thyroid differently than other hormone systems in the body.
In fact, it’s almost unfair in a way because we look at thyroid function differently than we do cortisol, estrogen, progesterone, and testosterone even though ALL of these hormones are regulated in a similar way to your thyroid.
It’s actually very easy to understand so let me explain.
This is how it works:
Your pituitary produces pro-hormones which then go act on different organs in your body and cause the release of specific hormones.
For the thyroid, your body produces TSH (thyroid stimulating hormone) which stimulates your thyroid gland (the organ) to produce thyroid hormone.
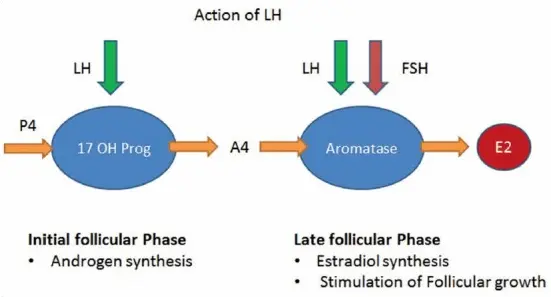
For estrogen and progesterone, your body produces FSH (follicle stimulating hormone) and LH (luteinizing hormone) which act on your ovaries (the organ) to produce estrogen and progesterone (2).
For cortisol, your body produces ACTH (3) (adrenocorticotropic hormone) which acts on your adrenal glands (the organ) to produce cortisol.
Do you see the pattern here?
Almost all of these hormone systems work in a VERY similar way.
They all are influenced by the pituitary gland and result in the release of very important hormones.
It would make sense then that we would evaluate each hormone system for problems in the same way.
But we don’t.
When it comes to your thyroid gland, we look directly at this TSH number and use that number as a way to estimate how well the gland is functioning.

For ALL other hormone systems here we nearly completely disregard the pituitary equivalent pro-hormone and instead look directly at the absolute concentration of hormones in the body.
This may not sound like a big deal, but it can have profound consequences.
For instance:
By looking at the TSH as a marker of thyroid function we are making the assumption that whatever outside forces we use to “alter” this number (usually thyroid medications) results in the same physiologic consequences as whatever your body does when it is producing thyroid hormone normally.
But how can we make that assumption when no other hormone system works that way?
When doctors give patients insulin they don’t give patients the exact amount of insulin that the pancreas produces normally. They alter the required amount of insulin based on the NEEDS of the patient (4).
And that’s what I propose we do for thyroid patients, even though we currently don’t.
Let’s take a look at other hormone systems to give you a better idea.
Let’s Look at Birth Control Pills
Birth control pills are probably the worst offender.
These pills contain synthetic hormones which are designed to completely shut down the normal function of estrogen and progesterone.
They do this by completely suppressing FSH and LH in your body (5), which are your pituitary pro-hormones.
FSH and LH can be compared to TSH because they all cause the release of their specific hormone from their target organ.
As you know, it’s a big no-no to suppress the TSH if you are treating with thyroid medication, but this is completely ignored if you are taking birth control pills!
In fact, if you tested any patient taking birth control pills you would find that both their FSH and LH are likely suppressed down to an undetectable level.
If we treated birth control pills like we do thyroid hormone then doctors would start with a small dose of birth control and then titrate the dose based on the FSH and LH.
Would it surprise you to know that doctors rarely even check the FSH and LH once they start taking birth control pills?
Do you know how they know if they are working or not?
They usually look at a clinical symptom which is the absence of the menstrual cycle as an indicator that the dose is just right.
If you aren’t having your cycle then the medication is “working”.
When we apply this same concept to people on thyroid medication, that is that we increase their dose until their symptoms disappear it is considered malpractice.
Doctors will tell you that the reason we don’t suppress TSH is that it can lead to negative consequences.
But the only consequences they cite are bone loss (6) and risk of atrial fibrillation (7).
I’ve already written about how the science isn’t settled in that lowering the TSH definitely results in these conditions and you can read more about this idea here if you’d like.
And if we are using the same logic, we might ask ourselves, “does suppressing the FSH and LH with birth control pills also cause any problems”.
And the answer is most likely, yes.
Newer studies are showing that using birth control pills may increase your risk of certain types of breast cancer (8).
In addition, there are probably other consequences that should be considered such as weight gain and consequences from excess synthetic estrogen.
The thyroid system is somewhat different from the estrogen/progesterone system in that all medications used to treat thyroid conditions are considered “bio-identical” or exact replicas of the same hormone that a normal healthy body produces.
None of our current iterations of birth control pills are considered bio-identical, in fact, they are all slightly manipulated synthetic versions of estrogen or progesterone.
This means that we can’t compare both therapies and consequences, but it’s still a very interesting exercise to look at both of them together.
And, by the way, when women go off of the pill they also tend to experience a rebound rise in FSH and LH (9) which is similar to what thyroid patients experience when they stop taking thyroid medication.
Let’s Look at Steroids
Next on the list are steroids.
And by steroids, I am referring to cortisol.
Cortisol is perhaps more closely related to thyroid hormone when compared to estrogen and progesterone simply because both cortisol and thyroid hormones are required to sustain life.
Having incredibly low levels of both cortisol and thyroid hormone in your body may lead to death.
So you can imagine that doctors take low cortisol very seriously and rarely ever prescribe cortisol unless it is absolutely necessary.
But do you know how doctors test for low cortisol?
They look directly at your serum cortisol level (first thing in the morning).
If both the thyroid and cortisol systems were the same then we would determine if you have enough cortisol by looking at your ACTH level and then prescribe the dose of hydrocortisone based on that.
But that’s not what we do at all.
In fact, it’s the exact opposite.
Doctors know that prescribing even SMALL doses of steroids results in complete suppression of the ACTH (10).
And, as you might imagine, the ACTH plays a minimal role in helping to determine the dose needed.
But, unlike estrogen and progesterone, doctors do care a little bit more about the ACTH because it impacts how long it takes for a patient to recover.
The longer you take steroids (synthetic or hydrocortisone) the more suppressed your ACTH will become and the longer it takes for it to recover after you stop taking your medication.
For this reason, doctors never let people who have been on steroids for longer than 1 month stop taking their steroids cold turkey.
Instead, they prescribe a “taper” dose which allows them to lower their dose slowly over time.
This gives their body (and HPA system) time to recover.
This same phenomenon occurs when you start taking thyroid hormone as well, but your thyroid system seems to recover faster than your cortisol system.
So, despite the similarities between your thyroid system and your cortisol system, they are both treated completely differently.
Let’s Look at Testosterone
Next on the list is testosterone.
And for this section, I’m going to focus mainly on men, even though the same logic applies to women.
When a man goes into the doctor’s office to test his testosterone level how do you think it’s done?
It’s done by testing DIRECTLY for serum testosterone levels (both free and total testosterone).
It’s NOT done by testing for the LH or FSH (which would be the same logic used when testing your thyroid).
In addition, once a man is being treated for low testosterone his dose is titrated based on the absolute concentration of testosterone in his blood, not the LH or FSH.
If we applied this logic to your thyroid then we would care a lot more about your absolute thyroid hormone concentration (which can be tested by looking at free t3, and free T4, by the way) and a lot less about your pituitary pro-hormone TSH.
And, much like estrogen and progesterone therapy, the FSH and LH in men taking testosterone are extremely suppressed.
In fact, even low to moderate doses are enough to shut down the HPA system and reduce FSH and LH to undetectable levels.
It appears that while the pituitary system is great for managing your sex hormones, thyroid, and cortisol on its own, it’s exquisitely sensitive to outside forces or hormones.
We can and should use this information when we look at your thyroid.
Do your Free T3 and Free T4 Have Value?
The question is:
Why do doctors not care about free thyroid hormone levels and instead focus on TSH?
The answer is that they don’t believe that free T3 and free T4 have any value.
And that’s a big problem because there is emerging evidence to suggest the exact opposite.
For instance:
#1. Newer studies (from 2017) have shown that free thyroid hormones are a better predictor of weight loss when compared to TSH (11).
People who have higher free T3 and total T3 levels tend to lose more weight than those people with low free T3/total T3.
This is a problem when you realize that doctors don’t care what your free T3 is so long as your TSH is fine, but it’s very possible for you to have both a low free T3/total T3 and a “normal” TSH.
If the TSH is the best measurement of thyroid function then why doesn’t the TSH track with weight loss when compared to free thyroid hormone levels?
The answer is because it’s not the best marker.
#2. In addition, there are genetic variants that are now documented and known which alter how well a person can metabolize or break down thyroid hormone.
Certain individuals, no matter how much thyroid medication they take, will NEVER be able to produce enough T3 thyroid hormone on medications like Synthroid if they have this genetic variant (12).
How can you compare someone with this genetic variation to someone who doesn’t have it?
You can’t, and the only way to know if someone has it is by testing free T3 and total T3.
And, by the way, there are plenty of other genetic variations which influence how your body responds to thyroid medication.
In the near future, we should be able to run your genetics to determine how well you might respond to the various types of thyroid hormone medications.
#3. If that wasn’t enough, we also know that there are endocrine-disrupting chemicals that can influence free thyroid hormone levels without altering the TSH.
Certain chemicals, which you and I come into contact with on a daily basis, have been shown to interfere with normal thyroid hormone processing at the cellular level (13).
These chemicals look similar enough to thyroid hormone that they are able to sit on your thyroid hormone receptors.
This is a problem because then your normal thyroid hormones can’t activate cellular receptors because they are blocked.
And the only way for thyroid hormone to work is to hook onto these receptors and activate the cells.
You can imagine, then, that as these receptors are blocked your body will be in a state of relative hypothyroidism (depending on which cells are blocked) even though your blood tests are “normal”.
The only way to find out if this problem is occurring is by evaluating free thyroid hormone levels.
These are just a handful of documented reasons which should give physicians who use the TSH as a marker of thyroid function pause.
And, as a patient, you should also be aware of these because it will help you understand if your doctor is up to date with current literature or not.
If you are working with a doctor that doesn’t recognize these factors (for whatever reason), then you may want to seek out a second opinion from someone who is more up-to-date.
Surprisingly (or not), you will find that many doctors are behind new research by an average of 17 years or more (14), so it may take some work on your part to find those doctors who are actively reading new research.
Is Suppressing your TSH Dangerous?
I know that it may seem like I am advocating for the complete disregard of the TSH in favor of looking directly at your free thyroid hormones but that’s not my stance or my opinion.
Instead, my idea is that we should use a combination of lab tests to help us better understand what is going on with thyroid function in thyroid patients.
There are so many thyroid patients out there who are suffering from symptoms related to low thyroid function despite taking “adequate” amounts of thyroid hormone.
Doesn’t it make sense that we re-evaluate our current treatment paradigm to see if we missed anything?
I think TSH is an important measure of thyroid function, but it simply doesn’t give a clear picture of what is happening with the thyroid system.
How can it, when there are so many other factors at play?
Instead of focusing solely on the TSH, we should look at the TSH in conjunction with free T3 levels and free T4 levels.
While doing this, we should put preference on optimizing these free thyroid hormone levels even if it means slightly lowering or suppressing the TSH.
We should, however, not blatantly disregard the TSH and ignore it completely.
The TSH certainly has value and can help us understand how a patient responds to thyroid hormone and how high or low their dose may need to be.
Conclusion
Doctors place a huge emphasis on TSH when they evaluate thyroid function.
Even though the TSH can be useful, it may not be the best or most appropriate tool for diagnosing and managing thyroid problems.
If you are someone who is struggling with persistent hypothyroid symptoms DESPITE taking ‘adequate’ thyroid medications, then you may be someone who needs more advanced testing.
Not everyone will fit into this category, however, as some people may be perfectly fine when looking at the TSH.
But if problems arise during your treatment then the next step should be to look at your free thyroid hormone levels.
Now I want to hear from you:
Are you someone who is feeling poorly despite taking thyroid medication?
Do you have a normal TSH but still remain symptomatic?
Have you had your free thyroid hormone levels tested?
Leave your questions or comments below!








Dear Dr. Childs,
I have watched many of your great videos. I have a question about Papillary Thyroid Cancer. Do you know of any cases that have been successfully treated and/cured with Low Dose Naltrexone(LDN)in lieu of surgery? And if so, which doctors prescribe it?
Thank you!
Hi Kathy,
I do not. I wouldn’t really consider LDN a treatment for thyroid cancer. My personal opinion is that it would be very risky to avoid treating a treatable cancer such as thyroid cancer given the risk that it may spread. While it’s not optimal to remove your thyroid, you can absolutely still have a life if you find a doctor who will treat you with combination T4/T3.
Thank you so much for your reply, Dr. Childs. 🙂
Dear Dr. Childs,
This is a new field for me to explore. I am learning so much from your blog. Recently I have checked my TSH and it was 21.8 and in a month I have checked by blood again but with full thyroid panel: This time I had the following results (below). I am wondering if my TSH is just acting out or I have to do more investigation. I do not want to get on medication for the rest of my life. However, the doctors want me to start taking Levothyroxine 0.075MG. Thank you very much.
T3 UPTAKE 33 22-35 %
T4 (THYROXINE), TOTAL 6.4 5.1-11.9 mcg/dL
FREE T4 INDEX (T7) 2.1 1.4-3.8
TSH 11.79 mIU/L
Hi Kate,
I would take a look at this blog post for more information: https://www.restartmed.com/stop-taking-thyroid-medication/
It sounds like you probably also need to do some more investigating with further labs and a more complete personal history.
I’m curious what would be considered good conversion rate? My ft4 is 54% thru the range and ft3 45%. Do I convert ok or not? I have increased my levo but thinking about adding synthetic t3. TSH is still in the range but on the low side (0.76) Personally I don’t think much of TSH. It’s neither here nor there. Very poor indicator of thyroid function. How did doctors reduce the whole complexity of hypothyroidism to a single blood test that doesn’t even come from thyroid itself is beyond me.
Hi Kristina,
To get accurate information on conversion you also need to look at your reverse T3. That will tell the rest of the story. And I agree with you, it doesn’t make sense to look solely at the TSH for such a complex system, but here we are!
You can learn more here: https://www.restartmed.com/reverse-t3/
Hi Dr. Westin,
I had a total thyroidectomy in 2003 and have struggled with weight gain, exhaustion, mood swings, hair loss… I’m a walking Hypo textbook. A few weeks ago I got fed up with feeling this way and started to do some research, which is how I found this site. My Endocrinologist has refused to test anything BUT my TSH since I’ve been seeing him for the last 10 years. He disregards my complaints and tells me to eat less and exercise more (I diet AND exercise, btw). So the question is- do I just look for another doctor or do I try to discuss further testing with the current doctor? And if it’s the latter, how do I present that to him so that I will be heard?
Discovering your site has been both wonderful and hopeful as well as heartbreaking- heartbreaking to think that maybe I could have felt better for the last 10+ years of my life…
Any advice you could offer would be truly appreciated.
Many thanks,
Robyn
Hi Robyn,
Typically, it’s a better use of your time and energy to seek out a second opinion because most doctors are not willing to budge in their ideology and treatment philosophy even in the face of information contained on blogs and websites such as this. You can use this resource to help: https://www.restartmed.com/thyroid-doctor/
Hey Robyn,
I’m from Germany and my thyroid got removed because of Graves in 2011. I had two or 3 horrible years until I switched to t4 plus t3 medication. Its not perfect but much much better. Now I help others to do so if needed. Talk to your doctor with Dr Childs infos. My sister promised her doc a good bottle of wine if precribing cytomel and a second if working. He got both. And they were no good team before that.
Bring your t4 to to middle for t3 start, you might have to lower t4 a bit. Then you take 10 mcg of t3 in 3 portions, that is 3 mcg per portion throughout 24 hours. That will be a relief. From there, you can increase slowly further, and you dont have to keep every dose for weeks. Try to find a dose thats working relatively good and then keep and measure blood.
For me, its 137 t4 and 20 t3, latter in 4 doses throughout day. Many have 15 t3 and are ok.
No fear, you will get better soon !!! Regards from Germany, Anja
Thank you for such interesting and informative articles. When I was in my 20’s with good, PPO insurance, I had a doctor that diagnosed me with a lazy pituitary gland. Unfortunately, I was too young and naive to ask questions about it. In my 30’s, I started gaining 1 to 3 pounds per week. I saw my HMO doctor who told me to cut down on my calories, so I reduced my calorie intake to between 800-1000 per day and was still gaining weight. I saw the doctor again and he said I was eating more than I was admitting. My thyroid tests always came back normal. In 2008, I had a total thyroidectomy, followed by RAI treatment due to cancer. The Endo that I was assigned to put me on synthetic thyroid meds and I was always tired so she added Cytomel, which helped, but caused me to be jittery and gave me allergic reactions. My pharmacist told me to tell the doctor to switch me to Armour Thyroid and she didn’t want to, so I switched Endo’s. This new one is just like the last one. She goes strictly by the labs and not how I feel. I’ve asked her to test my Free T3 but she refuses. I can’t lose weight to save my life, I have several hypo symptoms, but she won’t help me because my TSH is repressed. She’s talking about reducing my dosage and I don’t know what to do. The symptoms, especially the fatigue, can be almost crippling. I’m not sure I can afford to see an Endo outside of my insurance plan. Any suggestions?
Hi Dawn,
Your best bet is to find a doctor who is more willing to work with you and who thinks outside of the box as outlined in this article. You can find more information on how to do that here: https://www.restartmed.com/thyroid-doctor/
Dr. Childs,
I have personal experience with being over-medicated by a primary car doctor who was only using TSH to treat me for Graves Disease. I have gone through three doctors in two years (including two endos), trying to find someone who will treat me accurately and consistently.
Through my own research, I have been able to better understand my results and have started ordering tests myself through an independent lab. I have also been able to stop taking medication by adjusting my diet (gluten, dairy and refined sugar-free) and adding a variety of supplements. However, I still have symptoms that feel mostly like hypothyroid but a little like hyper; and my labs are coming back with my TSH still below normal and my T3 and T4 on the low end of normal (which is not optimal for me at all).
My current endo wants me to stay off medications (which I prefer) and doesn’t seem like she knows whether to treat me as hyper or hypo – so isn’t treating me at all, in spite of my ongoing symptoms. And I don’t know whether to take supplements aimed at elevating or suppressing my thyroid function.
I’m wondering, based on another article of yours, if I should have my cortisol levels checked. I did live in fight-or-flight mode for about five years while escaping, divorcing and protecting my children from an abusive sociopath. So adrenal fatigue makes sense! I just know something is still not right, and I am not sure how to proceed.
Thanks, Elisa
Hi Elisa,
In my opinion, I think it’s often best to test serum cortisol when you evaluate your serum thyroid lab tests because these two hormone systems are linked. So, yes, that would be a reasonable approach.
My TSH is 1.30. free T3 is 2.7. Free T4 is 0.9 and reverse T3 is 14
I’m on 25mcg Liothyronine and 75mcg Levothyroxine which my doctor just increased to 100mcg Levothyroxine. I have Hashimotos and losing weight is practically impossible. I feel very discouraged.
Hi Eli,
I would take a look at these resources for more information:
– https://www.restartmed.com/lose-weight-hashimotos/
– https://www.restartmed.com/weight-loss-naturethroid/
Hi Dr Child’s
Have been underactive thyroid for 20 years. I have given up with my GP after 3 months of being unwell and being told my bloods are normal. (Pins & needles, fainting, panic attacks, anxiety, nausea) I have had 2 private tests done (results attached) through the post. After the first one I reduced my levothyroxine from 150mcg to 125mcg, but am a bit confused by the second results. Still not right but not as bad. Please note I have started HRT as also menopausal, and am taking cbd oil for the last 2 weeks which is helping with anxiety. What are your thoughts on the bloods? Is it better to reduce the TSH, and ignore the antibodies? I would be happy to continue with the blood tests, but need to be able to interpret results and change meds effectively. Thanks in advance.
Sue
Sorry just spotted I can’t attach results – is there a way I can do that?
Hi Sue,
In terms of looking at thyroid lab tests, some tests are more important than others but I would never just ignore any of the results.
Hi Dr. Childs,
I follow your blog and podcast and I was so glad to see this topic on why the TSH isn’t always the best test.
I am currently lucky enough to have been under the care of a practitioner who believes this. I was diagnosed with Hashimoto’s in 2010. Once I was on Nature Throid for about a year, my TSH became suppressed but my doctor understood it was not the end all be all. I was doing well. I lost 20lbs with diet and exercise. When I was pregnant, my OBGYN doctors repeatedly told me I had a “thyroid problem “ and my TSH was “too low” even though my T4/T3 was on the lower side of normal. They kept me on my dose but never increased. They were clueless. I am lucky my baby was fine. I had moved a few hours away and tried to see another local Primary doctor who said he was “holistic”. When he saw the suppressed TSH, he said that means I am on “too much” and kept lowering my Thyroid medication even though I had low T4.
I went from being on 4 grains per day and feeling great to 1 grain over 6 months. I kept complaining about excessive fatigue and weight gain to him despite going to Orangetheory 3 times per week. He had no answers and kept lowering. I had gained 12lbs (I am 5’2) quit Orangetheory after gaining weight and began getting Vertigo. I was dome. I called my old doctor and he agreed to see me over the phone. After labs, He immediately put me back on bio-identical Progesterone after my OB prescribed (Nora-Be) to treat low progesterone. He also put my Nature Throid dose back to where it was before I saw the last doctor. Within 6 months, I lost 10lbs without even working out just walking. I tried LDN for a short time and had positive results except for some nausea. I just started to try again at 1.5 instead of 3mg. I will print out your info in case I ever have this problem again. THANK YOU!
Hi Annette,
Awesome! Thanks for sharing your story and I’m glad that you are starting to feel better.
Dr. Westin,
I have had my thyroid removed due to cancer. Good news is that I am cancer free. I have gained about 20 lbs and I was already overweight. I have always struggled with low thyroid. I always had to run a high T3 to feel good. I currently take Natural Bovine Thyroid and a small dose of cytomel. My doctors freak out because I run a low TSH. If I take the amount of meds they recommend I know I am not getting enough. Is there a danger running a very low TSH after removal?
I have also suffered from adrenal fatigue. I had to take an early retirement due to stress.
My goal is to regain my energy and lose some weight. I would like to get off the cytomel and I think the combination of Thyroid Adrenal Reset and the T3 Conversion booster may help me. I really do not have a Doctor right now that is knowledgeable about thyroid issues. I use to have a Doctor but he is no longer a resource for me. I am use to adjusting my meds according to symptoms and have had good success in the past. The blood tests have never been a good indicator for me. I know I am not your patient but any advice you could give me would be appreciated. Thank you.
Dawn
Hi Dawn,
The short answer is that there are potential risks if you suppress your TSH. I would recommend you check out this article on that exact topic for more information: https://www.restartmed.com/suppressed-tsh/
TSH 0.01 mIU/L Low 0.40-
4.50
1
T4,Free 1.1 ng/dL 0.8-1.8
T3,Free 3.4 pg/mL 2.3-4.2
I take Armour thyroid 60 in the morning and 30 in the afternoon. I’m told my TSH is too low and should take fewer meds. Shouldn’t the tsh be low if I had thyroid cancer? I have constipation but am pretty good otherwise. I weigh 100lbs, 5’2″ and am 55yrs old. I have mild hot flashes and I wake a lot at night. Is that my age or my meds?
Thank you for your time
Laurie G
I have been on 150 mg of desiccated thyroid medicine for a few years, my doctor recently refered me to an endocrinologist who completely panicked when he saw that my TSH has been suppressed in my last few lab results (I’m talking a TSH of 0.00something), and he immediately cut my dose to 90 mg a day. However my free t3 was within range, the lab won’t test my free t4, my reverse t3 was 19 and I don’t have hyper symptoms. Since the endo has cut my dose I have gained weight, but he maintains I am hyper and need to get my TSH to climb back up or I’ll have a heart attack or something. What do you think ?
Hi SB,
I would take a look at this article for more information on that topic: https://www.restartmed.com/suppressed-tsh/
Great information!!! Thank you for educating all of us women who desperately need it. I know so many who are suffering and are seeing clueless Drs, and they won’t find a new one who is more responsible! I will try again to help them by forwarding this information to them.
Fortunately, I began seeing an in-tune NMD when I first moved back to Phoenix in 2011 with horrible hypo-thyroid and many other issues. Dr Kevin Barnett ordered all of the thyroid tests (which no one else did before)and put me on custom whole thyroid (due to my Celiac Disease). What a difference! Down the road since then I have also been diagnosed with Hashimoto’s and PCOS. Unfortunately, my CD was misdiagnosed when I was 4 yo, so 50+ years later I finally was diagnosed with CD and began to correct my food intake…but a lifetime of CD ravaging my muscles and bones, et al, has taken it’s tole and I’m playing catch-up while aging. Add an incident being dowsed with synthetic lawn chemicals and now being hyper-chemically sensitive makes my life a nightmare.
I now also see an OB/GYN who specializes in menopausal women (had a complete hysterectomy at 36 yo due to medical misdiagnosis), and who also is knowledgeable about doing ALL of the thyroid tests. Dr. Deborah Wickman has me on 60 mg NPThyroid (one of the few NDT’s available with incipients I can tolerate) which puts my TSH at 1.0 with the rest in alignment. My PCP Dr Danielle Wicklow is also in line with ordering all thyroid tests. Dr. Barnett originally, and now Dr. Wickman also have prescribed for me a custom hormone cream with C-Biest, progesterone, and testosterone that I call my anti-aging cream! I have found THE best compounding pharmacy at Phoenix Pharmacy on Thomas Rd in Phoenix – they are meticulous in their compounding and knowledgeable in what NDT products are available and what ingredients I can tolerate. I went through quite a few pharmacies before finding them.
Do you know what’s up with the unavailability of most of the NDT’s with only a couple of the synthetic T3 and T4’s available? This has been going on for several years now…a ploy by big Farma to cripple the Natural/NDT industry?
It took a lot of time and effort for me to find these amazing providers who keep up with research, and who LISTEN to the patient and respond accordingly! If other readers in Metro-Phoenix are searching for a 2nd opinion or need to change Drs I highly suggest trying them out.
Dr. Childs, your website is SO extensive with easily absorbed information, it has helped me immensely to understand more fully how my body works. My ONLY complaint is that I spend so much TIME reading your work….but that’s something that I consider an investment in my health!
Thank you so much!
You have an interesting and informative web site. Thanks for writing on this subject.
I’ve read that bones have TSH receptors so everyone needs to have some TSH to maintain bone density. I’m 65 so bone density is a concern. I had a total thyroidectomy 7 years ago for a fast growing benign nodule. I have a family history of aggressive thyroid cancer. It has been extremely difficult to find a thyroid dose that brings my TSH into the normal range while keeping my Free T3 and Free T4 mid range. That mid range Free T3 is very important for symptom reduction. My current endocrinologist is quite happy with my TSH of 2.1 and Free T4 of 0.82 (0.78-2.19) and Total T3 1.01 (0.97-1.69). She ran a Free T3 but it was not reported to me. If TSH is so important, why don’t doctors supplement with TSH when it becomes suppressed and the supporting labs are below range or low in range?
Hi MJ,
Many cells have TSH receptors but almost every cell has thyroid hormone receptors including your bone cells. So, while TSH receptors play some role, it likely pales in comparison to the role that thyroid hormone receptors play. It’s, therefore, easier to supplement with thyroid hormone than it would be with TSH. In addition, TSH supplementation would only work if your thyroid gland is working and because most people have primary hypothyroidism this means TSH supplementation would be ineffective.
I have problem with my TSH,just posted but not sure if it sent successfully
Hello Dr Childs,
I was diagnosed with hypothyroidism 14 years ago and just found out from my new doctor (an endocrinologist) that I was incorrectly diagnosed. He deterred this by requesting my original labs from 2008.
He also says I’m over medicated my TSH -0.001. T4 ~9
My concern is he suggested I either stop taking my medication cold turkey or only take it 3 days/week.
After reading your blog I’m very concerned that my endocrinologist isn’t giving good advice either. He’s also believes TSH is the “gold standard” for diagnosing thyroid dz.
I’m so exhausted from seeing doctors who don’t really understand how to manage this health issue. What do you recommend I do?
Hi Susan,
You will want to use this resource to help you find a competent thyroid doctor: https://www.restartmed.com/how-to-find-a-doctor-to-treat-your-thyroid/
Life is too short for you to continue to suffer and waste time going to doctors that aren’t willing to listen to you.